Contracted Deviated Nose Revision Rhinoplasty with Rib Cartilage
- Dr. Chayoung Kang
- 2025년 4월 30일
- 5분 분량
This case reviews contracted deviated nose revision rhinoplasty in a patient who had undergone four previous nasal surgeries and later developed an upturned nasal tip, nasal deviation, nostril asymmetry, and filler-related distortion. Surgery focused on residual filler removal, rib cartilage septal extension, nasal tip stabilization, nostril reshaping, dorsal realignment, and closed rhinoplasty reconstruction.
Author: Dr. Cha-Young Kang
Clinic: NoseLab Clinic
Published: 2025
Last Updated: 2026
Introduction
Hello, this is Dr. Cha-Young Kang of NoseLab Clinic.
This case involves contracted deviated nose revision rhinoplasty after four previous nasal surgeries. The patient presented with a retracted and upturned nasal tip, nasal asymmetry, deviated bridge, nostril asymmetry, and filler-related distortion along the nasal bridge.
The surgery was performed using a closed rhinoplasty / endonasal approach. The goal was to lower the upturned tip, correct nasal deviation, remove residual filler and foreign material, improve nostril symmetry, and rebuild nasal support using autologous rib cartilage.
Patient Background and Surgical History
The patient had a complex surgical history involving implant surgery, septoplasty, implant removal, dermal grafting, rib cartilage grafting, alar base reduction, additional tip revision, and filler injection.
Previous Surgical History
The surgical history included:
6–7 years ago: Silicone implant and ear cartilage rhinoplasty
5 years ago: Implant replacement and septoplasty
4 years ago: Implant removal, autologous dermis grafting, rib cartilage grafting, and alar base reduction
2 years ago: Nasal tip revision with rib cartilage
1 year ago: Filler injection for a low nasal bridge
After these procedures, the nose showed contracture, deviation, asymmetry, and filler-related contour distortion. Because the patient had already undergone multiple operations, the tissue condition and scar formation had to be evaluated carefully.

Initial Observations Before Revision Surgery
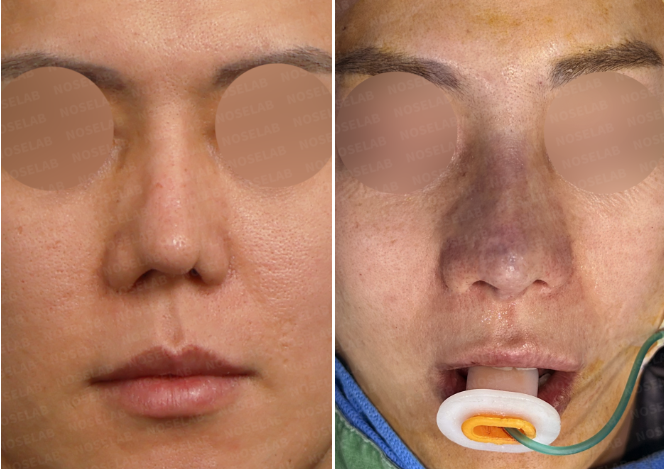
Preoperative design consultation photos were reviewed from the frontal, side, oblique, and nostril views.
Frontal View
The frontal view showed a crooked nasal bridge, bulky dorsal contour, bulbous nasal tip, and alar base asymmetry. The left nostril appeared smaller, suggesting asymmetric contracture and lower nasal imbalance.
Side View
The side view showed a high radix, drooping and retracted nasal tip, and a small nasolabial angle. The nasal tip position appeared imbalanced in relation to the upper lip and nasal bridge.
Nasal Base View
The nasal base view showed nostril asymmetry, pinching, and contracture on the left side. These findings suggested lower nasal structural weakness and scar-related distortion.
These findings indicated that the revision plan needed to address both the nasal framework and the surrounding soft tissue condition.

Patient’s Goals
The patient’s main goals were to correct the deviated bridge, lower the upturned nasal tip, improve nasal symmetry, and restore nasal projection.
Main Surgical Goals
The main goals included:
Correction of the deviated nasal bridge
Lowering of the upturned and retracted nasal tip
Improvement of nostril symmetry
Correction of nasal base imbalance
Removal of residual filler and foreign material
Improved nasal projection
More balanced dorsal and tip contour
The patient also requested dorsal support using a silicone implant. In this case, implant use had to be planned carefully because previous surgeries and filler injection had altered the tissue condition.
Surgical Plan for Contracted Deviated Nose Revision Rhinoplasty
The surgical plan focused on structural correction, filler and foreign material management, nasal tip support, nostril reshaping, and dorsal contour refinement.
Septal Extension with Autologous Rib Cartilage
Autologous rib cartilage was used for septal extension to support and reposition the contracted nasal tip.
This step was important because the tip needed to be lowered and stabilized after repeated previous surgeries.
Alar Repositioning and Nostril Reshaping
Alar repositioning and nostril reshaping were performed to improve nostril asymmetry and correct the pinched, contracted lower nasal appearance.
The goal was to create better balance between the right and left nostrils while respecting the patient’s scar tissue condition.
Dorsal Realignment
The deviated nasal bridge was realigned to improve the overall nasal axis. This was planned together with nasal tip correction because deviation can involve both the upper and lower nasal structures.
Nasolabial Angle Correction
The nasolabial angle was adjusted by repositioning and stabilizing the nasal tip. This helped improve the relationship between the nasal tip and upper lip.
Residual Filler and Foreign Material Removal
Residual filler and foreign material were carefully removed to create a cleaner foundation for reconstruction.
This step was necessary because filler-related distortion can interfere with dorsal contour and make revision rhinoplasty less predictable.
Controlled Silicone Dorsal Implant Placement
A silicone dorsal implant was used to improve dorsal height and contour. The implant was planned only after filler removal and tissue assessment.
The implant had to be positioned and shaped carefully to avoid unnecessary pressure on the nasal tip and surrounding soft tissue.
Surgical Results
Frontal View
From the frontal view, the nasal line appeared straighter and more balanced after correction. Alar asymmetry improved, and the lower nasal structure appeared more even.

Side View
From the side view, the nasal tip appeared more naturally projected after rib cartilage support and tip repositioning.

Nasal Base View
From the nasal base view, nostril symmetry improved after alar repositioning and nostril reshaping. The pinched and contracted appearance was reduced.

Structural Outcome
The nasal tip was stabilized with autologous rib cartilage support. Residual filler was removed, and the dorsal contour was reconstructed with controlled silicone implant placement.
Because this was a multiple revision case, the outcome was planned within the limits of scar tissue, previous surgical changes, and available soft tissue.

Surgeon’s Commentary
Revision rhinoplasty for a contracted and deviated nose after multiple previous surgeries requires careful planning. In this case, the difficulty was increased by prior implant surgery, septoplasty, dermal grafting, rib cartilage grafting, alar base reduction, tip revision, and filler injection.
The most important part of the surgery was to stabilize the lowered nasal tip using autologous rib cartilage. In contracted nose revision, the nasal tip often tends to return upward if the internal framework is not sufficiently supported.
Residual filler and foreign material were carefully removed to create a cleaner surgical foundation. This was important because filler-related distortion can affect both the contour and the accuracy of dorsal reconstruction.
Nostril asymmetry and pinching were addressed through alar repositioning and nostril reshaping. The deviated bridge was also corrected to improve the overall nasal axis.
This case shows that contracted deviated nose revision rhinoplasty should not be planned as a simple tip-lowering procedure. The nasal bridge, septal support, nostril shape, filler residue, scar tissue, and previous surgical changes all need to be considered together.
FAQ
Why can the nasal tip become upturned after multiple rhinoplasty surgeries?
The nasal tip can become upturned when scar contracture, tissue tightening, weak septal support, or previous cartilage changes pull the tip upward. Repeated surgery can increase the complexity of this problem.
Can a contracted and deviated nose be corrected together?
Yes, both problems can be addressed together when the surgical plan includes septal support, nasal tip repositioning, dorsal realignment, and nostril correction. The exact plan depends on scar tissue, previous surgical history, and tissue condition.
Why is rib cartilage used in contracted nose revision rhinoplasty?
Rib cartilage may be used when stronger support is needed to lower and stabilize the nasal tip. It can also help reconstruct the septal framework in complex revision cases.
Should filler be removed before revision rhinoplasty?
Residual filler may need to be removed when it causes contour distortion or interferes with surgical planning. Removal allows the surgeon to evaluate the true nasal structure more accurately.
Can nostril asymmetry improve after contracted nose revision?
Nostril asymmetry can improve when alar position, nasal tip support, and nasal base balance are corrected together. The degree of improvement depends on scar tissue and previous surgical changes.
International Consultation
For international patients, a photo-based consultation may help clarify whether contracted deviated nose revision rhinoplasty, rib cartilage reconstruction, filler removal, nostril reshaping, or dorsal implant correction may be needed.
WhatsApp: https://wa.me/821057360302

Home page : www.noselab.co.kr
Instagram : noselab_global
YouTube : Noselab
Email : noselab@naver.com


댓글