Upturned Nose Revision Rhinoplasty with Thin Nasal Tip Skin
- Dr. Chayoung Kang
- 2025년 5월 21일
- 6분 분량
This case reviews upturned nose revision rhinoplasty in a patient with thin nasal tip skin, visible cartilage outline, over-rotated nasal tip, nostril asymmetry, columella deviation, high radix, and functional nasal obstruction after previous silicone implant and ear cartilage rhinoplasty. Surgery focused on implant removal, rib cartilage septal extension, alar cartilage repositioning, skin reinforcement, fat grafting, synthetic dermal grafting, septoplasty, turbinate reduction, and nasolabial angle correction.
Author: Dr. Cha-Young Kang
Clinic: NoseLab Clinic
Published: 2025
Last Updated: 2026
Introduction
Hello, this is Dr. Cha-Young Kang of NoseLab Clinic.
This case involves upturned nose revision rhinoplasty in a patient who had undergone primary rhinoplasty 15 years earlier. The patient had thin nasal tip skin, visible cartilage outline, an over-rotated nasal tip, nostril asymmetry, columella deviation, and a high radix.
The surgery was performed using a closed rhinoplasty / endonasal approach. The goal was to reduce cartilage visibility at the nasal tip, correct the upturned shape, improve nostril balance, reinforce thin skin, and address functional breathing problems.
Patient Background and Surgical History
The patient had undergone primary rhinoplasty approximately 15 years earlier in Bucheon.
Previous Surgical History
The previous surgery included:
I-shaped silicone implant
Ear cartilage graft
Unknown history of septal cartilage use
After the previous surgery, the nasal tip skin became thin, and the nose developed an upturned appearance. The cartilage outline at the nasal tip became visible, and the nostrils appeared asymmetric.
Because the case involved both structural imbalance and thin soft tissue coverage, the revision plan needed to address the framework and the skin layer together.
Preoperative Assessment
Preoperative design consultation photos were reviewed from the frontal, side, oblique, and nostril views.
Major Aesthetic and Structural Concerns
The major concerns included:
Severely thin nasal tip skin
Visible cartilage outline at the nasal tip
Over-rotated and upturned nasal tip
Asymmetrical nostrils
Deviated columella
High radix
Wide nasolabial angle
Functional nasal obstruction
This was a complex revision case because both the structural support and the thin nasal tip skin had to be corrected at the same time.

View-by-View Analysis Before Revision Rhinoplasty
Frontal View
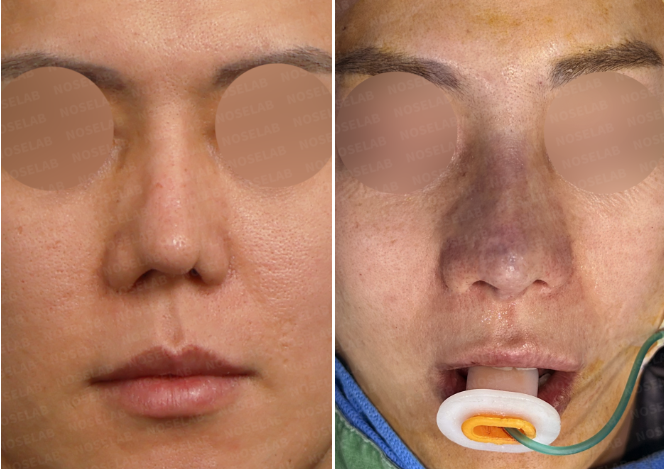
The frontal view showed an upturned nasal tip, visible nostril show, and asymmetry of the lower nasal structure.
Side View
The side view showed a sharp nasal tip, flat columella, wide nasolabial angle, and high radix. These findings created an over-rotated appearance.
Nostril View
The nostril view showed nostril imbalance and columella deviation. These findings suggested lower nasal support asymmetry and scar-related structural change.
The preoperative findings confirmed that the revision plan needed to include tip lengthening, skin reinforcement, columella realignment, nostril correction, and functional airway surgery.

Surgical Goals for Upturned Nose Revision Rhinoplasty
The surgical goals were planned around both nasal shape and tissue condition.
Main Goals
The main goals included:
Reduce nasal tip cartilage visibility
Correct the over-rotated and upturned nasal tip
Improve nostril symmetry
Realign the deviated columella
Lower the high radix for better facial balance
Reinforce thin nasal tip skin
Improve nasal airflow through functional correction
Because the nasal tip skin was thin, the surgery required more than structural repositioning. Soft tissue reinforcement was also necessary to reduce visible cartilage edges and improve skin coverage.
Surgical Techniques and Material Selection
The surgery combined structural reconstruction, soft tissue reinforcement, and functional airway correction.
Septal Extension with Autologous Rib Cartilage
Autologous rib cartilage was used for septal extension to support the nasal tip and correct the upturned position.
This helped provide stronger internal support for tip lengthening and stabilization.
Removal of the Previous Silicone Implant
The previous silicone implant was removed to reassess the dorsal structure and reduce implant-related imbalance.
After removal, the nasal bridge and radix were evaluated to determine how much height correction was needed.
Alar Cartilage Repositioning
Alar cartilage repositioning was performed to improve nasal tip shape, nostril symmetry, and lower nasal balance.
This step was important because the upturned shape was related not only to tip rotation but also to lower lateral cartilage position.
Septoplasty and Turbinate Reduction
Septoplasty and turbinate reduction were performed to address functional nasal obstruction.
Functional correction was included because nasal airflow can be affected by septal deviation, turbinate hypertrophy, and internal structural imbalance.
Nasolabial Angle Correction
The nasolabial angle was adjusted by repositioning the nasal tip and improving columella support. This helped reduce the over-rotated appearance from the side view.
Radix Lowering
The high radix was lowered to improve the transition between the forehead and nasal bridge. This helped create better balance between the upper nasal bridge and nasal tip.
Fat Grafting at the Nasal Tip
Fat grafting was used at the nasal tip to improve soft tissue coverage in the area with thin skin.
This helped reduce the visibility of cartilage outline and soften the appearance of the nasal tip.
Synthetic Dermal Graft for Skin Reinforcement
A synthetic dermal graft was used to reinforce the thin nasal tip skin and help mask visible cartilage edges.
This step was important because the nasal tip skin had become thin after previous surgery.
Before and After Results

Frontal View
From the frontal view, the visible cartilage outline at the nasal tip was reduced, and nostril symmetry improved. The nasal tip appeared more balanced after structural and soft tissue correction.

Side View
From the side view, the nasolabial angle improved after nasal tip repositioning. The upturned nasal tip was lowered, and the nasal tip contour appeared softer after skin reinforcement.

Nostril View
From the nostril view, nostril balance improved, and the nasal base appeared straighter after columella realignment and alar cartilage repositioning.

Structural Outcome
The nasal tip was reconstructed with rib cartilage support and soft tissue reinforcement. Fat grafting and synthetic dermal grafting were used to improve coverage over the thin nasal tip skin.
Because this was a revision case with thin skin, the result was planned within the limits of the patient’s tissue condition, scar tissue, and previous surgical changes.
Surgeon’s Commentary

This case required a layered approach to both structural and soft tissue correction. The patient had thin nasal tip skin, visible cartilage outline, upturned nasal tip, high radix, nostril asymmetry, and functional obstruction.
In revision rhinoplasty, thin nasal tip skin can make cartilage edges or graft outlines more visible. For this reason, simply repositioning the tip may not be enough. The skin layer itself must be evaluated and reinforced when needed.
Autologous rib cartilage was used as the main structural support for tip correction and septal extension. This allowed the nasal tip to be repositioned and supported after removing the previous silicone implant.
Fat grafting and synthetic dermal grafting were used to improve soft tissue coverage at the nasal tip. These techniques helped reduce visible cartilage outline and soften the nasal tip contour.
Septoplasty and turbinate reduction were also performed to address functional nasal obstruction. In this case, the surgical plan needed to address both the external nasal contour and internal airway condition.
This case shows that upturned nose revision rhinoplasty with thin nasal tip skin should be planned as a combined structural, soft tissue, and functional correction procedure.
FAQ
Why can the nasal tip become upturned after rhinoplasty?
The nasal tip can become upturned when scar contracture, cartilage repositioning, weak septal support, or excessive tip rotation changes the lower nasal structure. Previous implants or cartilage grafts may also affect tip position.
Why does cartilage become visible under thin nasal tip skin?
Cartilage can become visible when the nasal tip skin is thin or when graft edges are close to the skin surface. Repeated surgery, tissue thinning, and scar changes can make this more noticeable.
How is thin nasal tip skin reinforced during revision rhinoplasty?
Thin nasal tip skin may be reinforced with soft tissue techniques such as fat grafting, dermal grafting, or other tissue coverage methods. The choice depends on skin thickness, scar tissue, and structural needs.
Why is rib cartilage used in upturned nose revision rhinoplasty?
Rib cartilage may be used when stronger support is needed to lower and stabilize the nasal tip. It can also help reconstruct septal support in complex revision cases.
Can breathing problems be corrected during revision rhinoplasty?
Breathing problems can be addressed when septal deviation, turbinate hypertrophy, nasal valve narrowing, or structural obstruction is present. Septoplasty and turbinate reduction may be included when needed.
International Consultation
For international patients, a photo-based consultation may help clarify whether upturned nose revision rhinoplasty, thin nasal tip skin reinforcement, rib cartilage reconstruction, septoplasty, or turbinate reduction may be needed.
WhatsApp: https://wa.me/821057360302
LINE: [LINE Link]

Home page : www.noselab.co.kr
Instagram : noselab_global
YouTube : Noselab
Email : noselab@naver.com


댓글